




Ovarian tumors in pregnan
Anna Markowska
 Affiliacja i adres do korespondencji
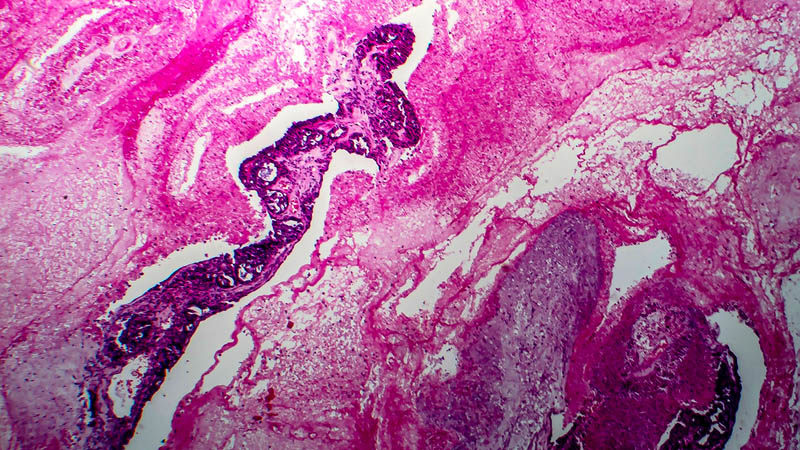
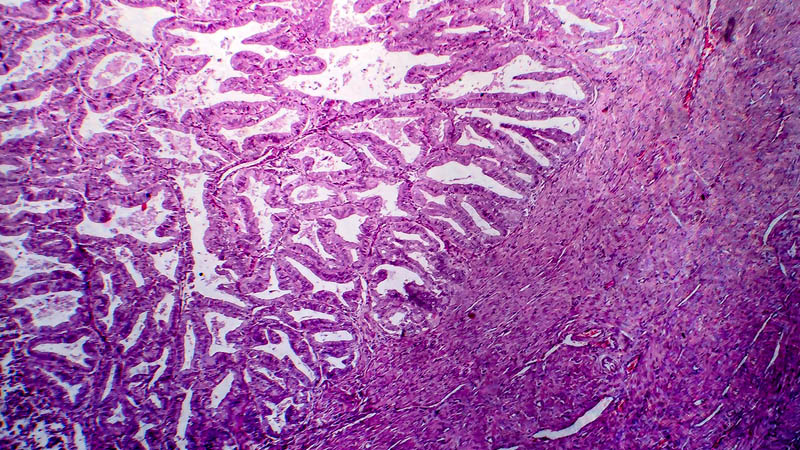
Affiliacja i adres do korespondencjiOvarian tumors develop in 2.3–8.8% of pregnant women. Most of them are benign cysts which vanish spontaneously after the 9th or 10th week of gestation. Ultrasound examination and magnetic resonance imaging are helpful diagnostic tools. Computed tomography, however, is contraindicated. The most common benign lesions are teratomas and cystadenomas. Malignant tumors account for 2.15–13% of all ovarian tumors in pregnant patients. Germ cell tumors, followed by borderline tumors and ovarian carcinomas constitute the most common ones. The management in the case of germ cell and borderline tumors involves unilateral adnexectomy and in invasive ovarian carcinomas, the treatment is individualized. In stage 1A G1, the management is similar to the one in borderline tumors and restaging after the delivery may be performed. Additionally, in early stages of carcinoma (stage IA G2 and G3, IB, IC as well as IIA), lymphadenectomy and platinum-based chemotherapy are recommended. In advanced stages, there are numerous possibilities of treatment including radical surgery with termination of pregnancy before the 20th–24th weeks of gestation and adjuvant therapy. Another option is the implementation of neoadjuvant chemotherapy during pregnancy and performance of cytoreduction following the delivery. At the mother’s request, delaying the treatment until after the delivery may be considered. Chemical treatment during pregnancy does not exert negative effects on the fetus provided that it is applied in the second or third trimesters. One of its rare complications is intrauterine growth restriction (IUGR). The survival of patients with ovarian carcinomas diagnosed during pregnancy is not different than in the case of women diagnosed without being pregnant.
