




Cervical cancer during pregnancy. Diagnostic problems and potential complications
Robert Jach, Małgorzata Radoń-Pokracka, Wojciech Kolawa, Paweł Basta, Marcin Mika, Marzena Kula, Monika Kabzińska-Turek, Antoni Basta
 Affiliacja i adres do korespondencji
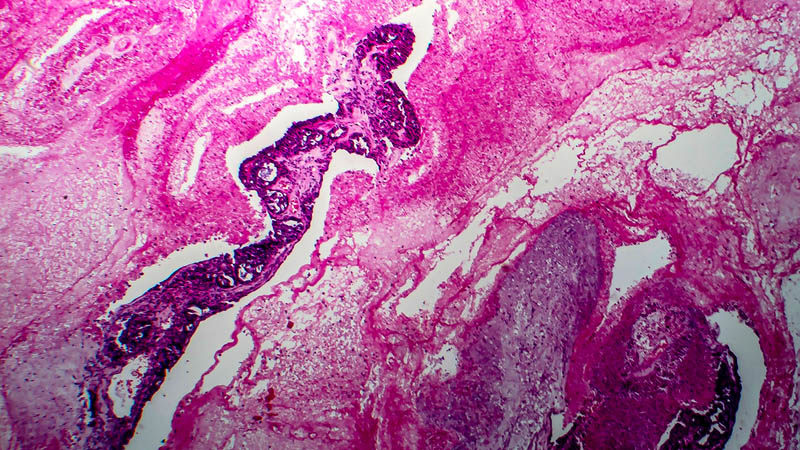
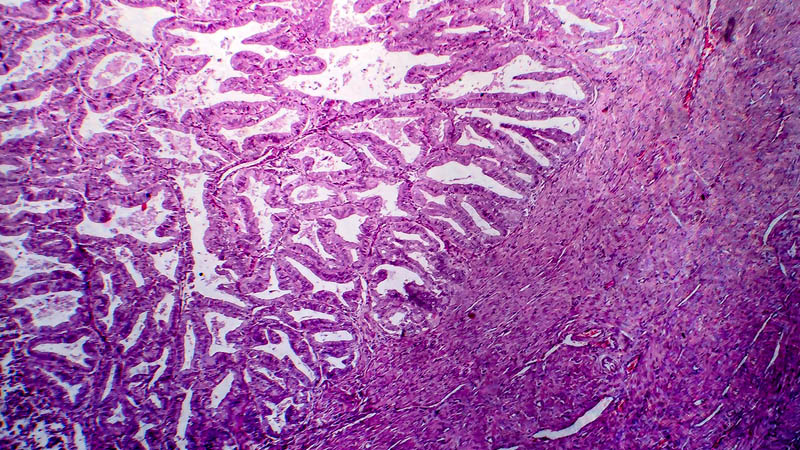
Affiliacja i adres do korespondencjiInvasive cervical cancer is the type of malignancy occurring most often during pregnancy and the incidence thereof is estimated at 1:1200 to 1:2200 cases. In the course of pregnancy, early stages of this tumor are usually detected. Typical symptoms of cervical cancer, i.e. vaginal bleeding, fluor and pain are highly non-specific and may be misdiagnosed as pregnancy-related phenomena. Oncologic and cytological diagnosis are an important component of prenatal care. When cytological study in a pregnant woman proves suspicious, the recommended modality for further diagnostic work-up is colposcopy. The main duty of a healthcare professional faced with a pregnant woman with pathological cytological findings is to exclude (or confirm) stromal invasion. Usually, close colposcopic-cytological supervision is recommended, and in the case of suspected stromal invasion – cone biopsy of the cervix. During pregnancy, cervical biopsy and conization of cervix are reserved for cases where invasive disease can not be ruled out by any other method, e.g. cytology, colposcopy or imaging studies. Imaging diagnosis should be implemented for the sake of clinical staging only and be limited to modalities associated with the lowest possible dose of ionizing radiation. Methods of choice include magnetic resonance imaging and ultrasonography. Curettage of cervical canal is not recommended. Diagnostic work-up requires vast experience and sound clinical judgment on the part of the examiner, enabling differentiation of pathological lesions from pregnancy-related physiological conditions. Progression of preinvasive disease to invasive stage during pregnancy is extremely rare. Studies confirmed possible regression of CIN lesions after termination of pregnancy. Chances for regression correlate with type of delivery, increasing after vaginal delivery. Pregnancy does not influence the course of disease at invasive stage, does not alter its prognosis or clinical characteristics. Caesarean section is recommended only in the case of suspected invasive cancer. There are few studies dealing with fetal complications associated, precluding any general conclusions. However, studies revealed an elevated proportion of newborns with low birth weight born by mothers at an invasive stage.
