




Neoadjuvant chemoradiotherapy in advanced vulvar carcinoma
Ryszard Krynicki1, Agnieszka Nalewczyńska1, Bogusław Lindner2, Magdalena Kowalska1, Beata Śpiewankiewicz1
 Affiliacja i adres do korespondencji
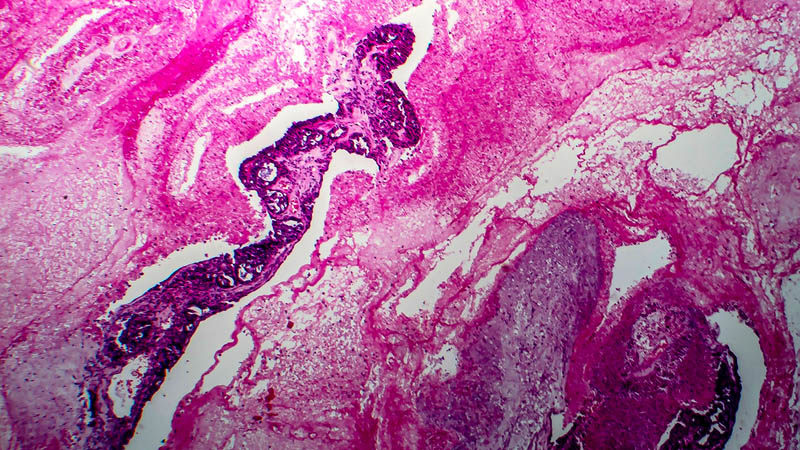
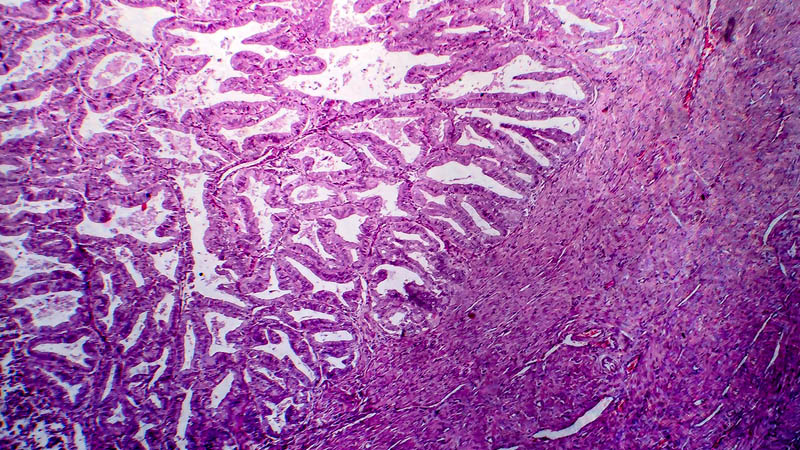
Affiliacja i adres do korespondencjiIntroduction: In advanced vulvar carcinoma with unresectable lesions, permanent curing is rare. In the past, extensive exenteration surgeries offered a chance for improvement but led to considerable mutilation and impairment of functioning. An alternative method of treating advanced vulvar carcinoma is neoadjuvant chemoradiotherapy or sole chemoradiotherapy. At present, chemosensitivity of vulvar carcinoma is well-documented. The application of synchronous chemotherapy with total dosage reduction by 15–20% in relation to radiotherapy allows for obtaining a favorable diagnostic index. The aim of the study was to determine the position of chemoradiotherapy in preoperative treatment of vulvar carcinoma. Material and methods: From 2005 to 2013, radiation therapy was applied in 24 patients aged 48–81 (mean age was 64) with squamous cell carcinoma of the vulva in FIGO stage III and IV. The therapies were conducted in the Department of Gynecologic Oncology of the Marie Skłodowska-Curie Memorial Cancer Center and Institute of Oncology in Warsaw (Poland). The patients’ vulvar region as well as inguinal and pelvic lymph nodes were irradiated with 15 MeV photons and/or 9–15 MeV electrons. The total doses used on vulva ranged from 54 to 65 Gy depending on the extensiveness of the infiltration. The dose used on the pelvic and inguinal lymph nodes ranged from 45 to 65 Gy. Chemotherapy: 750–1,000 mg/m2 of 5-FU administered as a 96-hour infusion and 50–75 mg/m2 of cisplatin on day 1 administered in the 1st and 5th weeks of radiotherapy. Results: Complete regression was obtained in 11 (46%) patients, partial regression in 12 (50%) patients and in 1 (4%) case, disease progression was observed. After the surgery, no carcinoma was detected in 3 (25%) out of 12 patients with partial regression; merely post-radiation damage was found. The instances of relapse were treated surgically and when the patient had not given consent or when the progression of the disease prevented surgery, systemic treatment was applied. Conclusions: In advanced vulvar carcinoma, neoadjuvant chemoradiotherapy with a high proportion of response should be a method of choice. Regression of carcinoma after irradiation allows for performing less mutilating surgeries. For optimal treatment selection, a decision concerning qualification for treatment in advanced vulvar carcinoma should be made together by a gynecologic oncologist and radiotherapist.
