




Placental site trophoblastic tumor – case report
Adam Cieminski, Agnieszka Januszkiewicz, Janusz Emerich
 Affiliacja i adres do korespondencji
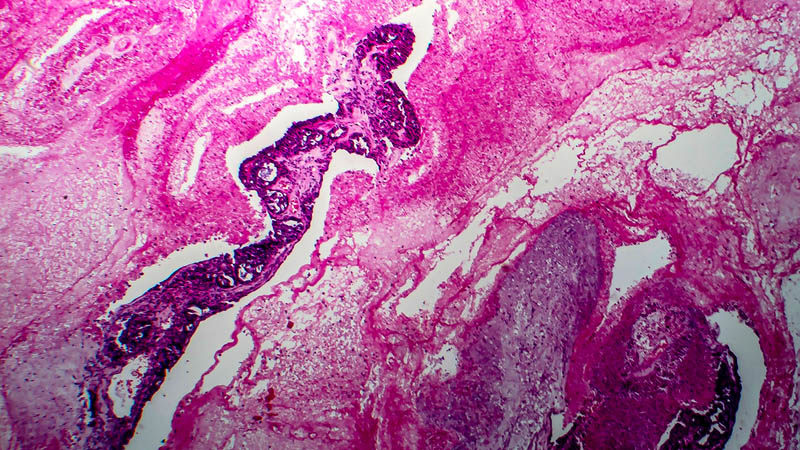
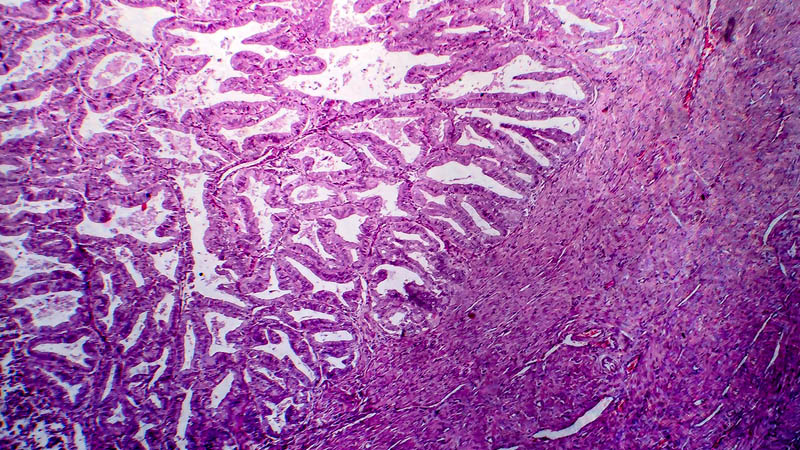
Affiliacja i adres do korespondencjiPlacental site trophoblastic tumor is the rarest and most difficult to diagnose forms of gestational trophoblastic disease. It constitutes 1–2% of gestational trophoblastic disease cases. The most common symptom of placental site trophoblastic tumor is abnormal vaginal bleeding with enlargement of the uterus. Symptoms related to the location of the metastases may occur as well. Placental site trophoblastic tumor may develop in women of any age after pregnancy as well as a long time after menopause. Placental site trophoblastic tumor mostly follows normal delivery, then molar pregnancy, spontaneous abortion, termination of pregnancy or ectopic pregnancy. Placental site trophoblastic tumor etiology is not entirely known. Inactivation and disregulation of TP53 gene as well as upregulation of EGFR and MIB-1 are thought to be the leading factors in the pathogenesis of this tumor. The tumor histologically arises from the intermediate trophoblast cells, which are present at fetus implantation. The majority of placental site trophoblastic tumor behave in a benign fashion and approximately 10–15% are clinically malignant. Placental site trophoblastic tumor can metastasize. The most common site of metastasis are the lungs and vagina. Placental site trophoblastic tumor is characterized by high human placental lactogen levels and high or normal human chorionic gonadotropin levels. The diagnosis of placental site trophoblastic tumor is confirmed by a histopathological and immunohistochemical report. Placental site trophoblastic tumor is usually resistant to chemotherapy. For this reason, placental site trophoblastic tumor is mostly treated surgically, including hysterectomy with or without adnexectomy and subsequent chemotherapy is administered. The first-line chemotherapy regimen is EMA-CO. For EMA-CO refractory cases, second-line chemotherapy is EMA-EP. Radiation is reported to be useful. In post-treatment monitoring, the chorionic gonadotropin and placental lactogen concentration in the blood is observed, as well as performing imaging examinations such as ultrasound, magnetic resonance imaging and positron emission tomography. The chance of recovery depends on the tumor advancement, time passed from the previous pregnancy and pregnancy duration as well as mitotic index of the tumor cells. In cases when placental site trophoblastic tumor is limited to the uterus, the prognosis is relatively good, providing hysterectomy has been carried out. Some cases of long-term remission have been reported with multiagent therapy.
